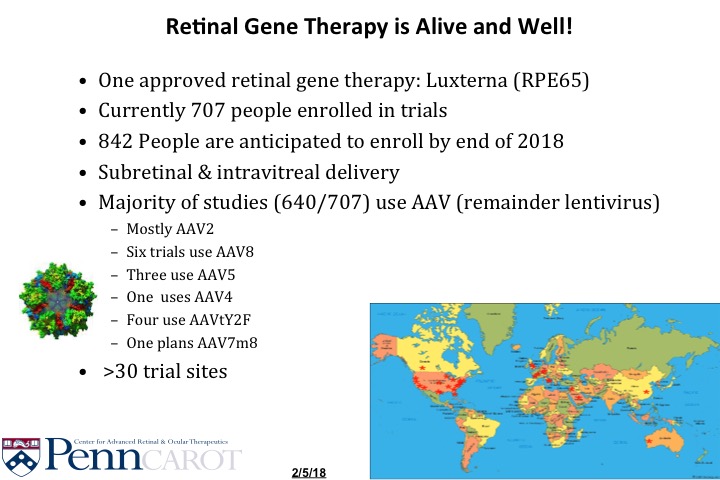
Since its launch in March 2018, breakthrough gene therapy LUXTURNA®™ continues to be successful in helping improve vision in people with inherited retinal disease due to mutations in both copies of the RPE65 gene and viable retinal cells as determined by a healthcare professional. The therapy treats LCA2, known as LCA/RPE65, one of more than 25 forms of Leber congenital amaurosis.
The drug – developed by Spark Therapeutics and a team of retinal research superstars that included Dr. Katherine A. High and Dr. Jean Bennett – came to fruition after 12 years of research and millions of dollars in investment.
Spark Therapeutics could not comment on the number of people who have received the gene therapy, but spokesman Kevin Giordano recently said the company has shipped well over 200 vials of the therapy since the U.S. Food & Drug Administration approval in December 2017. One vial of the drug treats one eye.
Trained retinal surgeons at one of the 10 eligible treatment centers in the United States deliver the gene therapy to the back of the eye by subretinal injection using a needle the size of an eyelash; about a week or so later, the patient undergoes the procedure in the other eye.
Read: 10 US Centers Offering Treatment
“Spark Therapeutics is thrilled patients continue to benefit from LUXTURNA (voretigene neparvovec-ryzl),” Giordano, Spark’s External and Product Communications Lead, said. “A gene therapy is a major milestone, not only for those of us at Spark, but also for the patient community and broader gene therapy field.”
The cost of the drug – $425,000 for each eye – initially caused anxiety among patient families, but Giordano had good news about insurance coverage.
“Payer coverage has exceeded expectations, and to our knowledge no treatment-eligible patient has been denied treatment due to their insurance coverage,” he said.
LUXTURNA also is being used beyond this country through license and supply agreements with Novartis, which has the rights to commercialize the drug in Europe and all other markets outside the United States. Spark manufactures and supplies the gene therapy to Novartis, according to Giordano.
Also, results from ongoing studies continue to support the drug’s safety profile and efficacy.
“In 2019, Spark presented four-year durability data from the LUXTURNA Phase 3 clinical trial,” Giordano said.
Read: LUXTURNA safety information
For privacy reasons, Spark Therapeutics cannot share patient results.
But we can – at least a couple of them because they came from patients and families sharing their stories with us.
For Hannah, ‘Hope Realized’
Hannah Reif, daughter of Amy and Chris Reif of Maple Glen, PA, underwent LUXTURNA gene therapy in July 2018. Dr. Albert M. Maguire, who is married to researcher Dr. Bennett, performed Hannah’s surgery at Children’s Hospital of Philadelphia (CHOP).

“We closely watched the clinical trials and the FDA approval process for seven years, starting when Hannah was diagnosed with LCA/RPE65 at just a few months of age,” Amy said. “Seven years of hope.
“Two years out from Hannah’s surgery, I can say we feel grateful and fortunate that she was treated with LUXTURNA. No regrets. LUXTURNA was hope realized. It delivered what it promised.”
She said what that has meant for Hannah has been nothing short of life changing.
“It has given her more independence, which has been wonderful for her self-confidence. It has given her the ability to see what she couldn’t before.”
Since the surgery, Hannah’s vision in dim lighting and her visual acuity improved. She is now 9 and just finished third grade.
Sometimes, her mom said, it’s the little things that are the most amazing.
“A year after the surgery, she was about to eat hot oatmeal and said, ‘Hey, I see steam. Hey, I can see that,’ ” Amy said.
“There are still things that pop up that she’s seen for the first time, like when she said, ‘Mom, did you know there’s a pattern on this toy?’ It’s fun to see her discovering.”
Amy said she and her family will be forever grateful to Dr. Bennett.
“There has been a lot of talk about heroes recently and Dr. Bennett is our hero. We are grateful for this groundbreaking treatment that she developed, that has been life-changing, not only for our daughter, but also for the sons and daughters and loved ones of so many others as well.”
‘His Vision Changed Everything’
Creed Pettit, one of the first recipients LUXTURNA, received the gene therapy at age 9 in March 2018. Dr. Audina M. Berracol performed the surgery at Bascom Palmer Eye Institute in Miami, Fla.
His mom, Sarah St. Pierre Schroeder, told us that her now-11-year-old is doing amazing and only occasionally has issues with dim lights, “but nothing like before.”
Their days in Mount Dora, Fla., have changed in a major way.
“He still starts his day with his trusty smoothie and waffle, but after that, Creed wants to create new pranks (today was putting ice in the tub). He said it was nice and warm so I could soak my feet.”
Creed now loves to play board games – Trouble, Sorry, Battleship and Uno.
“His vision has changed everything. He can manipulate small objects, he is using pointer fingers, and loves trying to roll his eyes in the mirror.”
Creed still likes to draw, and he loves riding and popping wheelies on his bike named Carlitos. He also likes to talk.
“Talking more is an understatement! Sunup to sundown, he is talking. He has also learned how fun it is to use his imagination, something he never did before. He creates awesome stories during this time. He is so much more independent; I have to remind myself of that often.”
At first, she and her husband, Chad, could see that Creed’s vision improved some, but once he became confident about his gene replacement, they noticed him finding toys and games.
“He was suddenly enjoying things he didn’t before. He now expresses when he can’t see. Yesterday it rained all day, I kept waiting for him to tell me it was too dark inside, but he was fine. He just started doing staring contests. I love looking at his eyes during the contest.”
Sarah said she is incredibly grateful.
“Creed’s surgery is something we still thank God, St. Raphael, St. Lucy and Sister Miriam Teresa, for every night.”
Like many kids across the country, Creed finished school at home because of the coronavirus pandemic. He graduated from fifth grade and thought because he finished school at home, he wouldn’t have to wear the graduation cap.
“But I was not going to let that slide,” his mom said. “I made one and took pictures.”
Anxiety, and a Friend to Call On
Throughout his journey, though, Creed felt anxious, something Sarah had learned that might happen when, before Creed’s surgery, she talked with Tami Morehouse, a LUXTURNA clinical trial participant at age 44.
Tami, a Sofia Sees Hope Ambassador, tries to calm fears and advises potential gene therapy patients and their parents that even though undergoing the surgery has the potential to do such good by improving vision, they should think about their expectations, especially with children.
“We are comfortable in our own zone; give us a little bit of change and it can throw us off,” Tami said.
Sarah understands.
“He started to have a lot of anxiety. He had a hard time sleeping. I feel everything changed so fast that he was overwhelmed, but we have worked hard on getting past that.”
Sarah and her family are in a great place now. But after they were home from the hospital in Miami and settled into their routine, she said she became very emotional.
“All the tears I had held in for nine years started to come out. I felt I no longer had a purpose; I was so used to staying busy. I did not know who I was supposed to be.”
She got some help and realized she still was needed because people need her help learning about and understanding this groundbreaking gene therapy.
“I still find myself shocked over how this has changed Creed’s life and so many other lives.”















{kind=link}
{kind=link}