Theodor Karl Gustav von Leber would be proud. So would Adolphe Franceschetti and Carl-Henry Alström.
Their research from the 19th and 20th centuries laid the foundation for groundbreaking gene therapy to treat Leber congenital amaurosis (LCA) and other rare inherited retinal diseases (IRDs). Translational research focused on LCA helped bring forth unprecedented numbers of genetic clinical trials now underway for IRD treatments and cures.
Dr. Tomas S. Aleman, associate professor of ophthalmology and director of the Hereditary Retinal Degeneration Clinics at the Perelman Center for Advanced Medicine and the Center for Advanced Retinal and Ocular Therapeutics at the University of Pennsylvania, discussed the beginnings of research into retinal degeneration as part of his presentation at the Hope in Focus (formally Sofia Sees Hope) second LCA Family Conference in Philadelphia last summer.
Dr. Aleman joined three panelists in a conference session called “One Disease, Many Approaches,” moderated by Brian Mansfield, PhD, executive vice president of research and interim chief scientific officer for the Foundation Fighting Blindness.
In a research paper published in 1871, Dr. Theodor Karl Gustav von Leber recognized early-infancy severe retinal disease with pupils that are “amaurotic,” related to amaurosis, meaning dimming, darkening, dark or obscure. Amaurotic pupils do not relate to light normally, expanding and contracting more slowly than normal or not responding to light at all. A large group of early-onset inherited retinopathies causing blindness carry his name as Leber’s Congenital Amaurosis.
“His descriptions still endure,” Dr. Aleman told his audience of more than 80 people from across the country and Mexico.
The evolution of research
Dr. Adolphe Franceschetti authored more than 500 articles throughout his life (1896-1968), realizing the retinal origin of the blindness and working on ocular genetics, Dr. Aleman said. A specific behavior comprised of poking, pressing and rubbing the eyes with a knuckle or finger to mechanically evoke perception of light is called Franceschetti’s oculo-digital sign and is characteristic of LCA. Researchers suspect this behavior in affected children may contribute to deep-set eyes and keratoconus, a condition in which the normally round cornea thins and bulges into a cone-like shape, causing distorted vision.
Dr. Carl-Henry Alström confirmed that LCA is genetic in nature, and he is credited with recognizing in the 1950s syndromic forms of LCA and other early-onset retinopathies such as Bardet-Biedl Syndrome, a rare genetic disorder with highly variable symptoms that may include retinal degeneration, obesity, reduced kidney function and many other features.
LCA occurs in 1 in 30,000 to 1 in 80,000 people and makes up 5 percent of all retinal dystrophies. Twenty percent of children with visual impairment and attending special schools have LCA.
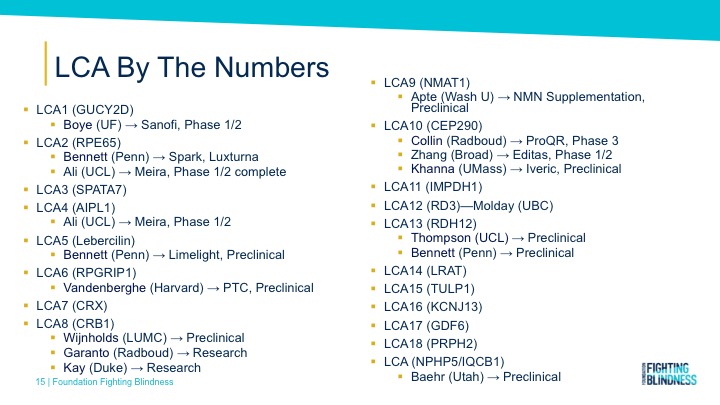
LCA, thought of as one disease until 40 years ago, now consists of more than 27 forms.
“It’s a large pack of diseases,” Dr. Aleman said.
Decades of work toward success
He characterized LCA as a molecularly heterogenous or diverse group of diseases with most primary disease location within the cells that perceive light or photoreceptors. Dr. Aleman detailed the complexities of clinical exams, vision testing and the spectrum of severity of vision loss observed in LCA. One such scenario, known as structural-functional dissociation, occurs when the loss of vision is disproportional to the loss of photoreceptors and is frequently seen in LCA, particularly very early in life. Such scenario represents the ideal for gene corrective treatment strategies.
RPE65-LCA studies led by a group of researchers at the University of Pennsylvania dating back to the late 1990s solidly demonstrated LCA could be treated. Dr. Aleman cited the importance of the translational research and clinical trials that led to federal approval of LUXTURNA™, a gene therapy treatment for LCA2 or RPE65-LCA, saying other, more frequent and neglected diseases have gotten attention through the RPE65 story.
He singled out two researchers, Jean Bennett, MD, PhD, who joined him on the conference panel, and her partner in research and marriage, Dr. Albert M. Maguire. He pointed out that their foresight and drive pushed research beyond the initial gratification granted by the spectacular results of early multi-institutional RPE65 gene therapy trials, to fulfill the practical need of an approved treatment for use in the clinic. The treatment, which produces dramatic gains in visual sensitivity, is the first and is, to date, the only gene therapy product approved for clinical use for an inherited retinal disease in the United States and Europe.
More patients have been treated with LUXTURNA since its approval in December 2017 by the U.S. Food and Drug Administration than those who received the medication during the clinical trials.
“I like to think that if it wasn’t for Jean and Albert, we wouldn’t be where we are today,” he told the gathering of patients, patient advocates, family members, researchers, doctors and biotechnology leaders.
No cure yet; work continues
Having one retinal gene therapy approved for use in the clinic, 900 patients enrolled in trials across 30 sites, and progress on therapies for the most severe forms of LCA, Dr. Aleman said, “That should stimulate ourselves to continue.”
He noted that much work remains to be done: LCA has not been cured, and researchers do not have a solution for every type of LCA. Gene therapy may not be enough for every patient or form of LCA, and the potential outcomes after treatments should not be expected to be the same across the heterogeneous group of diseases under the LCA umbrella.
In closing his presentation, Dr. Aleman posed three questions regarding LCA treatment and research:
- Can we treat hereditary retinal degenerations/LCA? “Yes, the answer is yes.
- Can we defeat LCA? “And the answer is also yes.”
- Do we have the tools and people to do it? “The answer is also yes.”
Dogs as test cases
In her presentation, Dr. Jean Bennett described how the RPE65 gene, when mutated, causes LCA2 or RPE65-LCA. In early research, Briard herding dogs that carried the mutated gene gained improved vision after receiving subretinal injections of an engineered virus of the human RPE65 gene. The treatment works by encoding an enzyme that converts light into electrical signals interpreted by the brain.
Dr. Bennett was one of the first investigators to use viral vectors, in which a virus is used as a vector or carrier that is genetically engineered to deliver the gene to specific cells in the retina. She is professor of ophthalmology at the Center for Advanced Retinal and Ocular Therapeutics and the F.M. Kirby Center for Molecular Ophthalmology at the Perelman School of Medicine. Please see a related story detailing her conference presentation.
Pam Stetkiewicz, PhD, vice president of program management at Editas Medicine, described a different approach using gene editing technology developed by Editas. The treatment uses molecular biology to create genomic medicine that precisely edits – by locating and removing – the targeted mutation in LCA10 or CEP290-LCA. She said the technology builds on the foundation inspired by Dr. Bennett’s gene replacement therapy.
More treatments in the works
Editas Medicine, based in Cambridge, Mass., in partnership with Allergan, based in Dublin, Ireland, use CRISPR/Cas9 gene-editing technology to accomplish DNA editing. The treatment, called EDIT-101, cuts out the mutation and is delivered to photoreceptors by subretinal injection. The editing permanently corrects the original, non-functioning protein essential for vision.
Dr. Stetkiewicz said Editas hopes to use the medicine to treat LCA10. Additionally, the company is developing experimental medicines to treat Usher Syndrome 2A and Retinitis Pigmentosa, among other IRDs. Editas is also working to develop engineered cell medicines to treat cancers and blood diseases, including Sickle Cell Disease.
The FDA approved the company’s 10,000-page data package, securing the required Investigational New Drug (IND) application to begin clinical studies with EDIT-101 in humans.
Editas and Allergan currently are recruiting patients with CEP290-LCA for a natural history study that will create the basis to test safety and efficacy in the Phase 1/2 clinical trial of EDIT-101.
Dr. Stetkiewicz said preclinical data shows that EDIT-101 is well-tolerated, efficacious and safe. Measurement of editing intended DNA versus unintended DNA is called specificity. Human retinal explants, pieces of tissue cultured for growth, treated with EDIT-101 resulted in a high level of intended editing with zero unintended editing, meaning the treatment has an excellent genomic specificity profile.
“So, we’re thrilled with this result,” she said.
Phase 1/2 clinical trials will begin in the second half of this year with 18 patients age 3 years and older at clinical sites in Massachusetts, Florida, Oregon and Michigan.
DNA, RNA, & LCA
Panelist Michael Schwartz, M.S., MBA, is vice president of ophthalmology at ProQR Therapeutics and is the global project leader for Sepofarsen (QR-110), an RNA therapy under development.
ProQR, based in The Netherlands with offices in Cambridge, Mass., is developing an antisense oligonucleotide (AON) product, Sepofarsen (QR-110), designed as a disease-modifying therapy for LCA due to the c.2991 +1655A>G mutation (p.Cys998X) in the CEP290 gene. The company is developing AON products, which are RNA therapies primarily for ophthalmic inherited disease. AON are short, single-stranded RNA molecules that interact with messenger RNA to prevent translation of a targeted gene.
Sepofarsen works like genetic tape to block the mutation p.Cys998X in the CEP290 gene.
To help understand what this means, Schwartz presented background on DNA, RNA and LCA:
The body comprises many different cells, and we have DNA in each of these cells. DNA contains many instructions for making all the different proteins, which are important building blocks needed by a cell.
When the cell needs a building block, it first copies instructions to a shorter blueprint called RNA; the RNA is then used to guide how to make a new protein, like CEP290. Together, these different proteins make sure the cell works as it should, resulting in normal vision.
But things don’t always go right. Inherited diseases are caused by mistakes in the DNA, and then these mistakes are copied into the RNA, as in the p.Cys998X mutation in CEP290.
This means that the proteins also will have the mistakes in them. They can’t work properly, and the cell cannot function as it should. This is what causes LCA.
He also detailed the workings of RNA therapies, saying they consist of short RNA molecules, with the aim to repair the mutation in a patient’s RNA – without changing the DNA – and to restore the function of the protein and the cell to hopefully improve vision.
A normal CEP290 protein maintains cilium structure in the photoreceptors of the retina and enables normal protein transport to the photoreceptor outer segment.
The CEP290 p.Cys998X mutation creates an environment that results in an aberrant exon that disrupts the splicing code of genes by truncating the CEP290 protein, ultimately leading to the degeneration of the photoreceptor cells.
Sepofarsen, delivered by intravitreal injection, blocks the recognition of the aberrance, and that results in favoring production of normal protein.
“We can actually reverse the phenotype of that mutation,” Schwartz said.
ProQR is finalizing interim results of its ongoing Phase 1/2 trial involving 11 people from ages 8 to 44. Schwartz said most of the patients had clinically meaningful improvement. The company’s Phase 2/3 trial began, with the first patient dosed in April. The 24-month trial expects to enroll 30 patients.
He cited an exceptional patient responder in the Phase 1/2 trial in which an adult with only light perception vision before the trial could now read letters on the eye chart.
“They said they could see things out of the treated eye that they had not seen for decades.”