Had he received a more definitive rare disease diagnosis in 2003, Alan Gunzburg said he might not have lost so much vision and still might be able to drive.
In 2016 – 13 years after his initial diagnosis – the Greenwich, Conn., man learned his vision and hearing loss was caused by Adult Refsum Disease (ARD), a genetic metabolic disorder with symptoms that perhaps he could have staved off years ago through dietary restrictions.
Doctors initially diagnosed Gunzburg with retinitis pigmentosa (RP) – a rare inherited retinal disease (IRD) causing progressive loss of peripheral and night vision. Those are also symptoms of Refsum disease, which, if undiagnosed, can be life-threatening.
The disorder results in a buildup in the nerves and liver of phytanic acid, a type of fat found in certain foods. Other symptoms are loss of smell and hearing, numbness, unsteadiness, itchy skin, and shortened fingers and toes.
Gunzburg joined more than two dozen speakers who shared their stories during a Feb. 26 virtual Connecticut Rare Disease Day celebration sponsored by the National Organization for Rare Disorders (NORD) and the Connecticut Rare Action Network (RAN).
His story reflects the plight of many people living with a rare disease because the more than 7,000 rare diseases in the United States are just that – rare.
It’s difficult to correctly diagnose rare diseases when little information exists about them.
Some families living with rare disease find they must create their own advocacy avenues to educate the public and the medical community about diseases they’ve never heard of.
Gunzburg created the Global DARE Foundation with the mission of Defeating Adult Refsum Everywhere. His website gets the word out about the disease and gives information on symptoms, treatments, and research.
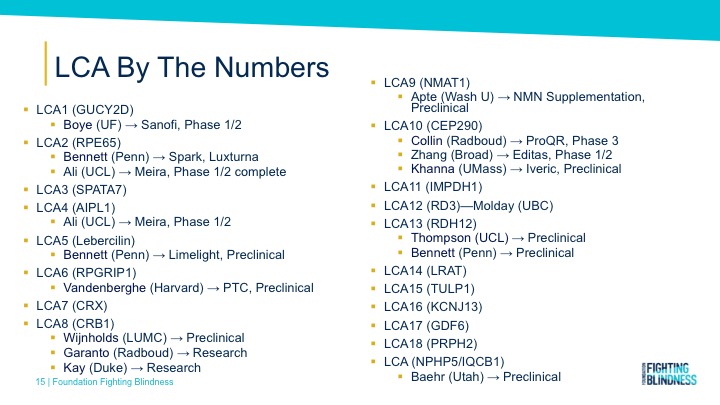
Laura Manfre, co-founder and board president of Hope in Focus (formally Sofia Sees Hope), took that same route in 2014 after doctors genetically diagnosed her daughter with a form of Leber congenital amaurosis (LCA). As a global patient advocacy organization, Sofia Sees Hope helps transform the lives of those affected by blindness caused by LCA and IRDs by generating awareness, supporting affected families, and raising funds to advance research for diagnosis, treatments, and cures.
Creating Rare Disease Advisory Councils
The global phenomenon of Rare Disease Day exists to create awareness of rare disease, characterized in the United States as affecting fewer than 200,000 people. With more than 7,000 rare diseases, 25 million to 30 million Americans are affected by rare disease. That means one in 10 Americans suffer from rare diseases, and more than half of them are children. The European Organization for Rare Disorders (EURODIS) organizes the international campaign.
Nationally, Rare Disease Day brings together each state’s RAN ambassador – in Connecticut’s case, Volunteer State Ambassador Lesley Bennett – along with patients, caregivers, doctors, advocates, legislators, academics, and business and biotech leaders to generate awareness, increase patient and caregiver support, and drive research for treatment and cures.
This year’s event focused on creating Rare Disease Advisory Councils (RDACs) in all 50 states through NORD’s Project RDAC. Councils are made up of various stakeholders, including patients, caregivers, doctors, insurers, biotechnology companies, researchers, and state officials.
Project RDAC’s goals are to optimize existing councils and increase the number of groups nationally by opening collaborative opportunities among councils, creating educational resources to guide them, and helping more states pass legislation that establishes high-functioning councils.
More than a dozen states have RDACs, 12 are pursuing RDAC legislation, and another 23 states do not have an RDAC.
Connecticut is working toward creating a permanent RDAC task force, after a temporary group disbanded in 2019. Check out this map to see if your state has an RDAC or if NORD is working on legislation to create one. To start an effort in a state, click here.
Telling Rare Disease Stories
NORD’s Kristen Angell moderated the virtual celebration that featured more than two dozen people, sharing stories about the struggles and successes in the world of rare disease. A recording of the celebration will be available soon.
Suzanne Candela literally told an uplifting story as outreach and mission coordinator for Patient Airlift Services (PALS) with the motto: “Going Above and Beyond to Lift People Up.”
Volunteer pilots help eliminate logistical barriers to treatments by using their own aircraft, fuel, and time to fly patients to appointments. Over the course of 10 years, the company helped 2,900 families in 23,000 flights, covering more than 5.4 million miles. Candela told of a girl flown from northern Maine to Boston for repeated cancer treatments. The patient has flown on PALS flights about 60 times and counting.
The service could eliminate transportation barriers for participants in out-of-state clinical trials. The company also has flown 900 flights bringing combat-wounded veterans to appointments.
Connecticut State Sen. Cathy Osten described the story behind proposed legislation that she and State Rep. Christine Conley introduced this session to help a local family struggling to pay for special food for their two children diagnosed with phenylketonuria (PKU). The family’s share of the cost is about $36,000 per child per year. Osten said insurance companies hesitate to pay but the expense is well worth it when it comes to the quality of life for people with PKU.
David Leeds of Avon has the rare disease Hereditary Angioedema with normal C1 Inhibitor (HAE-nC1Inh), a new form of hereditary angioedema (recurring episodes of swelling) identified in 2000.
If he goes to the hospital in this time of the COVID pandemic and no one knows about his rare condition and no one can speak on his behalf, Leeds said, “We just have to hope that my rare disease doesn’t kill me before they send me home.
“I have to know everything about my disease because my doctors don’t.”
John Hopper, one of the emcees of the virtual celebration, heads the Greenwich-based Fibrolamellar Cancer Foundation that advocates for people living with fibrolamellar carcinoma, a rare liver cancer that usually occurs in adolescents and young adults with no history of liver disease.
Hopper, who also co-chairs NORD’s Rare Cancer Coalition, said his strategy is to be what he calls “the mouse that roared.”
“That means we know we’re small, but we know we have to be loud,” Hopper explains on his foundation’s website. “Most people don’t know about rare diseases. Unfortunately, a lot of people don’t care about them. Our strategy is to be that loud voice – that leader – to make sure that every stakeholder from government to academia to pharmaceutical pays attention to this cancer and understands that working on this small cancer may lead to bigger things too for the rest of them.”
Hopper encouraged all the participants in the virtual rare disease day event to be that mouse that roars.











{kind=link}